
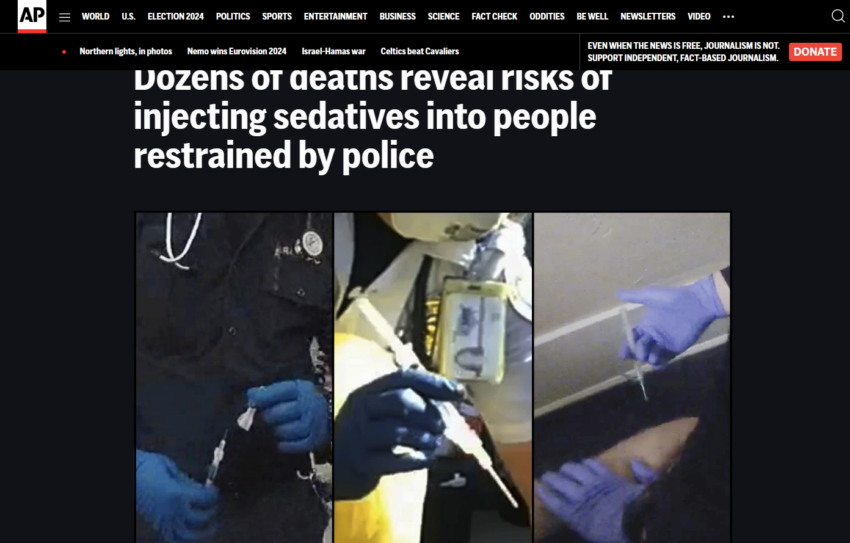
The AP recently published a story about EMS sedation of patients during police encounters — Dozens of deaths reveal risks of injecting sedatives into people restrained by police.
I was interviewed for it back in February of 2023, and the final story includes a small quote from me.
“I don’t believe he was a candidate for ketamine,” said Connecticut paramedic Peter Canning, who said he supports sedating truly violent patients because they stop fighting and are sleeping by the time they get to the hospital.
While I don’t believe that most in EMS sedate someone based on a request from police, I believe that it does happen. In the one case they showed me the video of, from what I saw, I don’t believe the patient needed to be sedated, much less held down and detained by police. He probably would still be alive today if the police had just left him alone.
The story cites numerous deaths of patients who have died post EMS/police encounter sedation – too many. It is hard to know the details of each case, but I wonder how many people died not because of the ketamine, but due to poor handling of the side effects of ketamine.
Benzos like versed, which Is what I have long used as my sedation drug –we only recently got ketamine and I haven’t had to use it yet for sedation- have the known side effect that it can put someone into respiratory arrest. Our answer in EMS has always been – but we can manage that. That’s why we carry ambu-bags and we have the ability to intubate if we need to. The problem with that is that it presumes that bag value mask ventilation and if needed intubation will be done well. That is not always the case. Some of these deaths may have been caused not by excess police pressure, but simple medical error. (Not being able to recognize/handle manageable respiratory distress/arrest). The end result though– the unnecessary loss of life–is the same. We need to be careful not only to only sedate people who truly need it, but to be cautious in our dosing and to weigh the risks. How easy will it be to manage this person’s airway? A thin person versus someone weighing 350 pounds with no neck may affect our choice. And to make certain if we do affect their breathing negatively, to recognize it quickly and take action. Anyone who is sedated needs capnography monitoring.
Kudos to the AP team for shinning a light on this issue and kudos to those EMS services that are using the story and some of these cases to review their procedures and training.
***
Below are excerpts from my correspondence with the AP reporter that further detail my thoughts on this issue.
Our questions:
- Was this man a good candidate for ketamine? We wonder whether he had already calmed down enough by the time he was injected, and whether he was showing “behavior with high probability of injury to patient or others” at the time of injection?
Based on the body camera footage, I don’t believe he was a candidate for ketamine. I would have liked to have seen them unhandcuff him and see if he cooperated or if he continued to fight. While still upset, he did not appear to be fighting his restraints or be a danger to anyone. At one point he even says, “I appreciate you,” to one of the responders. The ketamine was not given right away so EMS has plenty of time to access his danger level. That said, a couple of factors to consider. There were by my count six EMS people on scene, which suggests to me, not knowing the town or how EMS is done there, that there were two separate EMS/fire vehicles/crews. Maybe even from separate services. It does appear that a fire department paramedic (in the blue jeans, which I found odd) who may not have been with the original EMS crew is the one who gave the ketamine. In other words, I don’t think the first EMS worker we see, the woman, was in charge. She appears subservient to the man who later delivers the ketamine. I didn’t see a lot of discussion among the EMS people. There are two main categories of EMS providers – EMTs and paramedics. Paramedics can give ketamine, EMTs can not. I am betting the initial responders were EMTs.
Now, it is also important to understand the mindset of EMS when they arrive. Question: What were they dispatched for? The “unknown” or more likely for “the violent psych.” In other words, they may have some tunnel vision walking in, and the first thing I heard the police officer tell the female EMS worker was “He’s all over the place, he’s high on meth, tazed him twice.” I always go right to a police officer and ask them what is going on. I do that out of respect, as opposed just going right to the patient. I may disregard what they say, but it courtesy, just as when I arrive at the hospital, I expect the medical staff to ask me what I have before they start examining the patient. They can disregard what I say, but they should at least listen.
One of the parts that is most troubling to me is that had I seen what happened before he was tazed, I would have had a different impression than the impression the officer gives. Watching it, they told him (the victim) he wasn’t in trouble, he wasn’t doing harm. Where I work, if I get sent for a person acting strangely, if the person can tell me where they are and they can walk away, we usually, police and EMS, let them walk away. Maybe their local policy is you must have a name, but I think he could have walked away and none of what followed would have happened. There are a lot of people walking the streets on drugs not causing harm to others. He did not appear to be a threat to anyone other than he might have walked on another car.
- Was this too large of a dose of ketamine? Could this have played a role in triggering his cardiopulmonary arrest and contributing to his death?
Where I work as a paramedic, we only used Versed. As an EMS clinical coordinator, I oversee EMS services that use ketamine. Your first drug is versed, unless the person is extremely agitated, then you could use ketamine first. Our ketamine protocol is for 4 mg/kg round up to the nearest 50. No one gets more than 500 mg in a first dose. If you asked me to estimate the patient’s weight, based on the body camera I would also have said 80 kg so 400 by their protocol would have been a correct dose for the estimated weight, but not for the true weight. I will say it is common for people to overestimate a person’s weight, particularly if they are wearing layers of clothes. We have had cases where patients ended up needing to be intubated because they gave the patient too much ketamine for their weight, which turned out to be much less than estimated once the clothes were taken off. Once this patient’s jacket etc. was removed, he did look significantly less heavy than initially. A dose of 350 mg would have been more appropriate. Not certain it would have affected the outcome.
- Ketamine has been linked to adverse events that involve respiratory depression. The video shows that the medics had already given the man oxygen after he had repeatedly complained he couldn’t breathe. Should ketamine be given in such a circumstance?
Whenever someone says, “I can’t breathe,” you have to pay attention. I have heard that many times and it is never a good sign. It is not uncommon for people to be dismissive of someone in custody saying that. I have heard cops and EMS providers say, “Well, you can’t be having too much trouble because you are talking to me fine.” Ketamine can cause reduced breathing and weakness. If it does reduce the patient’s breathing, we have a cure for that, a bag-valve mask, and if needed intubation. We can effectively breath for the person should they need respiratory assistance. We can breathe effectively for them until the ketamine or Versed wears off. You don’t want to give them so much that they need respiratory assistance, but it is a side effect to watch for and be prepared to treat. I would say at this point his agitation is coming from his difficulty breathing not from the influence of drugs or psychosis,
I would hope that the crew put the patient on End Tidal CO2, which is required in our protocols for anyone who is sedated. If the person is entering respiratory failure, their ETCO2 numbers will start to rise, alerting EMS to a problem. If he died of acute hypoxic respiratory failure, the ETCO2 would have indicated this was a problem even before his oxygen saturation numbers went down, and before he went into cardiac arrest. Did they record his pulse saturations? I would also want to know what his initial heart rate was. Sometimes you can’t get these measurements before you sedate someone if they are truly still being violent, but you can try. I did not see them attempt vital signs. I deal a lot with people on PCP, and sometimes, my decision to sedate will be influenced by their heart rate. If they are fighting and their heart is going at 180, I want to get them calmed down. Someone with an enlarged heart, on meth, who has been tazered, and is still fighting is at risk of a heart attack and should be sedated. It is important to determine if someone is agitated due to hypoxia or psychosis. In either case, if they can’t be controlled, they need to be calmed down.
- Are there any concerns with the administration of ketamine after a subject is shocked with a stun gun and restrained in the prone position?
No, if a patient is violent and out of control, they need to be sedated. Sedation will enable them to be placed in a safer position, and their breathing monitored. As far as the prone position, a person should be kept in that only briefly if needed to control. I would have liked to have seen the police move him to a different position, but as it was, he wasn’t prone that long that I could tell. Again, on the ketamine. If you give ketamine and you follow it with proper care, that is fine, but if you give ketamine and don’t monitor the patient and don’t recognize impending respiratory failure and act to support their breathing, then that is a big problem. What kind of care did he receive in the ambulance? How long was he on the cardiac monitor until he suffered his cardiac arrest? What were his CO2 and pulse Ox numbers when first monitored? I also noticed he was still handcuffed when placed on the stretcher. I wonder when– or if — the handcuffs were removed. Our policy is to have the handcuffs replaced with soft restraints if restraints are still needed. They shouldn’t be if the ketamine is working. Otherwise, a police officer with a key to the handcuffs should accompany the patient in the ambulance, or at the minimum be following the ambulance. If the patient went into cardiac arrest while still in handcuffs and the handcuffs were not immediately removed that would have been a serious problem. Also, I think having his hands restrained behind his back certainly didn’t benefit his ability to breathe.
- Audio of the police officer in the second video shows him suggesting to medics and other officers a diagnosis of “excited delirium” at the 11:15 minute mark. At the 12:20 minute mark, the officer asks another “how long is it going to take for these guys (medics) to do something? Or are they just going to stand around and do nothing? So I said to him are you thinking this is an excited delirium case or what? Do you have anything to speed it up?” At the 14:20 mark, the officer says, “There we go! Looks like (medics) are here with ketamine.” At 15 minutes, the officer says, “when he gets poked, he’s not going to like that.” Are there any concerns with this type of pressure from police potentially influencing medical-decision making at a scene like this?
I don’t know whether the medic gave the ketamine in response to the officer’s comments or not. I couldn’t see his reaction. Such comments shouldn’t affect a medic’s decision to give ketamine or not. It is a while after that the patient gets the ketamine. Maybe the officer’s power of suggestion was an influence. I wouldn’t call it pressure. Another thing to keep in mind is that you don’t just walk up and inject someone with ketamine. Ketamine is a controlled substance so at least here in Connecticut, it is usually kept in a double-locked box in the vehicle, so a medic would have had to go back to the vehicle, get the vial out, get a syringe and a needle and draw up the proper dose, then return to the patient, or he would have had to have another medic do it. In some areas, the paramedic keeps the controlled substances on their person. That is what I do…Maybe one of the other medics had the drugs out. In either case, it takes a minute or two to get the drugs out, and drawn them up. Because he is not off the screen for long, I am guessing someone else may have drawn the drug up. I found it very hard with all the people crowding around the patient to see what was being done.
Another thought here is that I don’t think the police officer should really care if the patient gets ketamine or not. The person is being taken to the Emergency department not the police station. He is no longer the officer’s present concern. Once the ambulance leaves, he is in EMS hands. Whether he is tied down and fighting restrains or is sleeping on the stretcher due to sedation, the officer’s business, at least for now, is done. It doesn’t benefit him one way or another if the patient is sedated or not.
- What else did you observe that struck you? Anything else you want to add, either about this case or the general practice of sedatives given during calls with police involvement?
Bottom line for me on this case is from what I saw on the body camera, I don’t think he should have been sedated. I would have tried to get him on the stretcher, talked to him like a human being and seen if I could have calmed him down. I would have had his cuffs removed. Now it is common when I ask police to uncuff someone, they warn me that the patient may punch me. They may try to dissuade me, but they usually do what I ask, and if the person does suddenly become combative again, they are there to pounce on him again. As far as the ketamine causing his death, I don’t think so. If ketamine contributed to his death, it was the lack of provider response to what ketamine did that caused his death, not the ketamine. Could the enlarged heart, meth, tazer, and excitement have killed him by overloading his heart with more stress that it could handle, yes, that seems reasonable. But the hypoxia suggests to me his respiratory needs were not recognized. Maybe he was weakened and strapped too securely and couldn’t get full breaths. His continued agitation could have been due to increasing hypoxia. Again, ideally with ketamine, he would be calmed, his heart slowed down, his breathing better managed.
Final other thoughts. This is a pretty common scene. EMS shows up, person in cuffs, cops say the person is violent. And many times the person is truly violent and insane and a threat to himself and EMS. I have been in plenty of situations where I have had to wrestle patients who suddenly went nuts. I like chemically sedating violent patients because often instead of fighting them, watching them fight against restraints, spit and curse, they are sleeping like a baby by the time I get to the hospital. A note of caution, everyone reacts to sedation differently. I have given three doses of 5 mgs of Versed to a small woman until I could finally get her to stop fighting, and I have given 5 mgs to a large man and found myself having to grab my ambu-bag to breathe for him. The hospital is unhappy if you bring in a raving violent patient, and they are unhappy if you bring in someone obtunded from too much sedation. It is hard to get the right dose for the right person.
Overall, I think ketamine is a great drug. And there is a legitimate need to sedate violent patients. Like any drug, Ketamine needs to be used appropriately, and patients need to be monitored. Based only on what I saw on the body camera footage, I don’t believe ketamine was appropriate in this case.
According to federal EMS data, Ketamine was given 103,750 times in 2021. I don’t know how many times if was used for sedation as opposed to pain control or airway management. I don’t think there were many incidents like this one. I hope not as the video was hard to watch.