
“Addicts take opiates and other sedatives specifically to induce a pleasant stupor. If they’re lethargic and hard to arouse, but still breathing effectively, it’s not an overdose. It’s a dose.”
–Boston paramedic
This is a quote I included in a presentation I put together for the state of Connecticut back in 2014 when we designed a curriculum to teach BLS providers how to use naloxone.
Today, knowing what I know about stigma, I have altered the quote to:
“People take opioids and other sedatives specifically to induce a pleasant stupor. If they’re lethargic and hard to arouse, but still breathing effectively, it’s not an overdose. It’s a dose.”
The lesson we want to teach is just because someone is under the influence of an opioid does not mean they have “overdosed” and they need to be given naloxone.
Naloxone is for depressed respirations, not depressed mental status.
Opioid use alone (without depressed respirations) is NOT AN OVERDOSE and does not merit the use of naloxone.
To track the opioid epidemic, we track the number of overdoses, both fatal and nonfatal.
Fatal overdoses are easy to track. Patient is found dead, is suspected of opioid use and autopsy confirms opioids in the patient’s system. There is the possibility that someone may use opioids and die of something unrelated to the opioid use such as a heart attack or stroke and be called a fata overdose. At the same time many older people may die of opioid overdoses and responders assume the patient died of other causes. Their bodies are never sent to the medical examiner’s office and they are lost to opioid tracking.
Some states classify nonfatal overdoses simply as a patient who has received naloxone, and did not die. Sometimes this gets translated into each naloxone administration is a life saved.
That is not necessarily true. Some of the people who are given naloxone don’t need naloxone. They are dosed, not overdosed. The naloxone did not save their life and may have put them into painful precipitated withdrawal.
Some states classify an nonfatal overdose as any call that generated a 911 call as a result of opioid use resulting in altered mental status or depressed respiration, whether or not naloxone was ever given. A person “on the nod” who is resuscitated with stimulation is counted as an overdose.
Massachusetts does it differently and I think they are on to something.
Redefining and categorizing emergency medical service opioid-related incidents in Massachusetts
Massachusetts breaks EMS opioid incidents down as follows:
Category 1 (DEAD ON ARRIVAL) Deceased on EMS arrival. No resuscitation attempt. No hospital transport.
• Category 2 (ACUTE OVERDOSE [OD]) Patients who would have died without intervention, includes cardiac arrests transported to the hospital, and patients who received naloxone prior to EMS arrival, who are now recovering from initial condition.
• Category 3 (INTOXICATION) includes patients with opioid symptoms, who would have likely survived if medical intervention was not available. Includes patients who are lethargic, pinpoint pupils and on the nod.
• Category 4 (WITHDRAWAL) Patients seeking treatment for withdrawal symptoms or substance use disorder or entering a rehabilitation program.
• Category 5 (ORI OTHER) Includes suicide attempts in which opioids were involved and behavioral health-related with substance use.
You can view Mass data on their opioid dashboard. Click on severity Index.
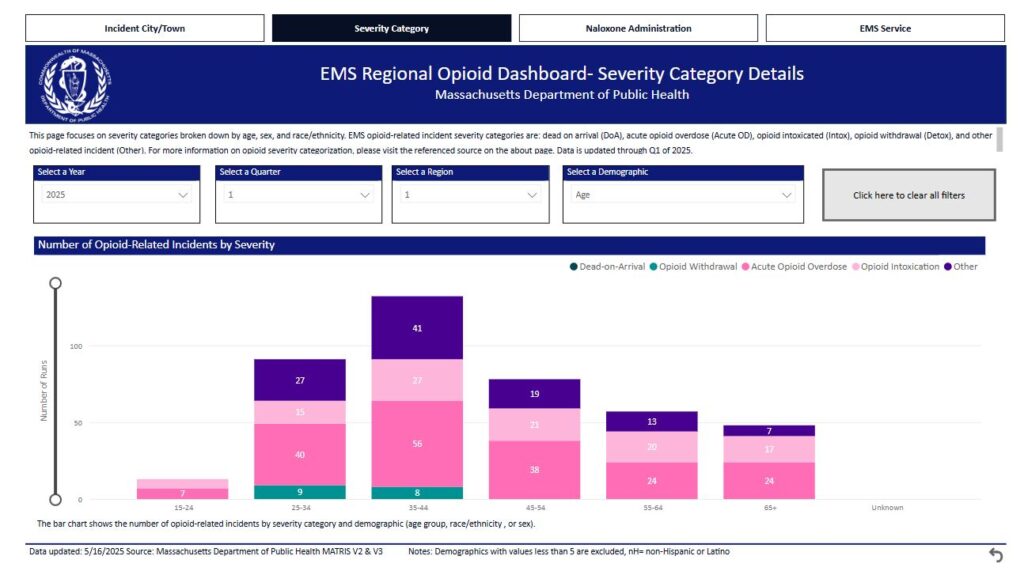
I think breaking it down into these or similar categories gives a much better picture of the epidemic and if tracked from month to month, sheds more light on what is truly happening with the epidemic than simple fatal and nonfatal.
I might modify their categories to these:
1. Fatal Overdose, includes dead on scene and those pronounced dead in the ED.
2. Acute Overdose: Patients unresponsive with depressed respirations requiring naloxone.
3. Intoxication: Patient with opioid toxidrome syndrome who are able to maintain respirations
4. Withdrawal: Patients experiencing withdrawal and/or those seeking opioid detox/treatment.